The bold, aggressive new plan released by Hillary Clinton once again wildly surpasses in ambition what U.S. officials dare attempt in this country.
This article was first published on December 1, 2012, in theAtlantic.com.
by Mark Harrington
On Thursday, outgoing Secretary of State Hillary Clinton released the Obama administration’s Blueprint for an AIDS-Free Generation, fulfilling a commitment she made at July’s International AIDS Conference for next-level global strategy to fight AIDS.
Unlike the earlier domestic U.S. National HIV/AIDS Strategy, released in 2010, the global Blueprint makes a bold scientific case, based on the latest science and buttressed by substantial progress from the field, that investments in high-quality combination HIV prevention efforts and treatments can dramatically reduce new HIV infections and HIV deaths, while saving millions of lives and billions of dollars.
The Blueprint even includes a mandate for research to end the epidemic, something lacking in less optimistic earlier plans.
The ambitious international goals set by the Obama administration on World AIDS Day 2011 appear likely to be met. The plan to use the President’s Emergency Plan for AIDS Relief (PEPFAR) and the Global Fund to Fight AIDS, Tuberculosis and Malaria to support ongoing treatment of 6 million people with antiretroviral therapy (ART) by the end of 2013, including 1.5 million pregnant women, is on track. Already 5.1 million people are on ART thanks to PEPFAR, of the 8 million total receiving these effective anti-HIV treatments globally. And in the past year alone, 750,000 pregnant women have received ART to prevent mother-to-child transmission of HIV, resulting in the births of 230,000 HIV-free babies.
What’s more, huge drops in the cost of generic drug manufacturing and improvements in health-care delivery systems meant that in 2012 PEPFAR was able to support twice the number on ART, 5.1 million, as it could just three years earlier with the same investment of approximately $5 billion.
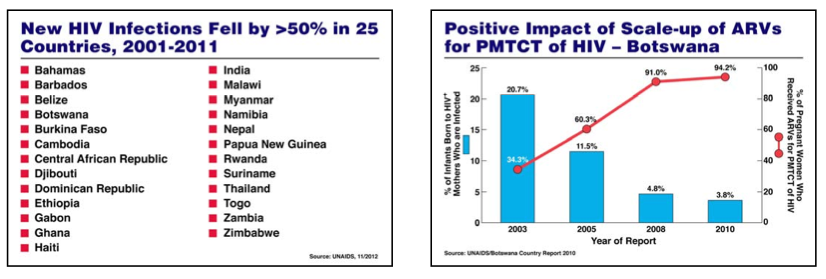
The report also reveals that — thanks to the Global Fund, PEPFAR, and increasing local investment — many countries have reduced their number of AIDS deaths by over 50 percent, including Botswana, Burundi, Cambodia, Côte d’Ivoire, Dominican Republic, Ethiopia, Guyana, Kenya, Namibia, Peru, Rwanda, Surinam, Zambia, and Zimbabwe. South Africa now has the world’s largest HIV treatment program, half of which is paid for with internal funds.
Some countries are even definitively putting the epidemic in reverse. Botswana, Ethiopia, Zambia, and Zimbabwe each put many more people on ART than were newly infected.
Other countries, such as Uganda, which have rising HIV infection rates, could achieve similar results by implementing high-quality combination prevention efforts (such as those focused on preventing mother to child transmission and encouraging voluntary medical male circumcision and condom use) and earlier treatment of those who are infected.
These results can be achieved in years, not decades.
Over the past decade, global HIV treatment has scaled up 200-fold, from 100,000 on ART in 2002 (mainly in Brazil), to over 8 million today. UNAIDS estimates that 14 million life-years have been saved globally by HIV treatment in the past decade, and almost 900,000 deaths averted this year alone.
Here at home, however, the epidemic is at a stalemate. New HIV infection rates have hovered around 50,000 per years for two decades — long before the introduction of effective HIV treatment. And the Obama administration is still committed to an under-resourced National HIV/AIDS Strategy. Not only is the U.S. plan not on track to achieve its goals, but they are themselves far less ambitious than what has already been achieved in the past decade in some of the world’s poorest countries, such as Cambodia, Ethiopia, or Zambia.
At a White House briefing which followed Clinton’s festive Blueprint launch, a diverse group of administration and community speakers discussed the domestic epidemic, but there were no new announcements save for Health and Human Services Secretary Kathleen Sebelius’ relatively anodyne tribute to the promise of the Affordable Care Act and its potential to help push forward the U.S. strategy, known by its acronym, NHAS:
Consistent with the goals of the NHAS, the ACA makes considerable strides in advancing equality for and helping people living with HIV/AIDS get the health insurance and care they need and deserve. When fully implemented, insurers will be prohibited from denying coverage to anyone or imposing annual limits on coverage – an important protection for people living with HIV/AIDS…. most private health plans must now cover HIV testing without a co-pay for adults and adolescents at higher risk and HIV testing and counseling for sexually active women. Medicare also covers certain recommended preventive services, including HIV screening for individuals at increased risk, without cost-sharing or deductibles. These preventive measures help people living with HIV/AIDS stay healthy while preventing the spread of HIV…. Because of the ACA, a series of investments to help providers support patients with chronic disease like HIV/AIDS are available. Under the law, states can receive extra federal funding to support high-quality coordinated care through Health Homes for Medicaid beneficiaries with chronic health needs. The goal of a Health Home is to treat the whole person, coordinating all their care from primary and acute care to behavioral health and long-term services.
Today, I am proud to announce that we will be issuing a rule to explicitly include HIV/AIDS on the list of chronic conditions that every state may target in designing effective Health Homes. This will make it easier for states to provide coordinated care for people living with HIV/AIDS.
Because the Supreme Court decision upholding the ACA turned Medicaid expansion from a mandate into a state option, the state-by-state struggle for equitable HIV treatment access will continue.
At the White House all speakers — Valerie Jarrett, Secretary Sebilius, PEPFAR’s Eric Goosby, and NIAID AIDS supremo Tony Fauci — expressed obvious relief that the election was over and that ACA implementation could proceed. Agreeing but broadening the point, a diverse and motivated group of community representatives spoke for young black women, young black gay men, Latinos, researchers, and providers. They cautioned that ACA implementation would not cover the needed housing, mental health, and other essential services required to deliver high quality HIV services.
It was good to be among a group of people committed to ending AIDS. But no one from the administration mentioned drug users. The ban on federal funding of needle exchange continues. No one mentioned the urgent upcoming need to reauthorize PEPFAR or the Ryan White Care Act, which will provide vital services, especially in states which decline to provide full HIV coverage under the ACA, and to provide community support, housing, and other services unlikely to be covered by insurance exchanges.
In the United States, only 25 percent of the 1.2 million HIV positive people are on effective ART with an undetectable viral load. Only 33 percent are retained in care. Only 82 percent even know their HIV status — a number that’s much lower among young people with the virus.
We can do much better. In nine years, Massachusetts has brought down its HIV infection and AIDS death rates by over 50 percent. Hospital costs dropped steeply over the same period.
On my way out of the gathering I ran into CDC Director Tom Frieden, who helped lead New York’s successful response to the HIV-associated, drug-resistant tuberculosis outbreak in the 1990s. I told him that with TB rates at a historic low in the United States, we were in danger of making the same mistakes which led to its outbreak in 1989 — excessive funding cuts, stockouts of first- and second-line TB drugs, inadequate political attention, funding and support. “TB is close to my heart,” he said. “You need to put it higher up on your agenda,” I replied.
Each year Obama has been president, he’s cut funding to the CDC and to the TB program.
It’s well past time for the administration to hold its own HIV/AIDS strategy to the same high standards that it expects from the scores of countries that have benefited from American generosity, and from their own increasing investments, to turn back the HIV pandemic in this decade.

{kind=link}